London Borough of Haringey: local authority assessment
Downloads
Overall summary
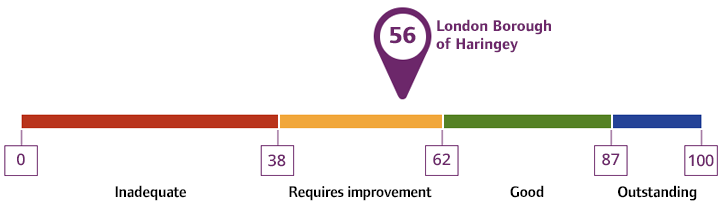
Local authority rating and score
Quality statement scores
Summary of people's experiences
People’s experience of the local authority’s services, care and support was mixed, with examples of both positive and negative outcomes.
Most feedback from unpaid carers was negative. This was related to the availability, quality and outcomes of assessments. Some carers told us support was not easily accessible or suitable and they did not feel supported in their caring roles. Carers who had access to an allocated worker told us their workers were responsive and supported them. Some carers told us getting a break was difficult. This was detrimental to their wellbeing and left carers at risk of breakdown.
People’s experiences of assessment, care planning and reviews was mixed. Assessments were broadly person-centred, strength-based and reviewed people’s needs holistically. However, timeliness of assessments and reviews were a barrier for people, with people facing long waits to be assessed or access support. Where people had accessed support, there were examples of positive outcomes for them. Contacting the local authority was also a barrier, with information not always being accessible. Communication needs were not always considered for people.
People had positive experiences of being supported by multi-agency integrated teams which enabled people to access services and stay independent. People were supported to access care provision within the local Integrated Care System (ICS) where in-borough provision was not available, but access to some provision was limited. This included day services and respite. There were mixed experiences of transitions between services such as Children’s to Adult’s services. Most people who used services felt safe but contact with people and partners following safeguarding referrals was not always consistent. People were receiving increased engagement through coproduction activities such as carers and coproduction groups.
Summary of strengths, areas for development and next steps
The local authority was undergoing a transformation to a locality-based model to improve their processes and better support communities. Senior leaders told us they recognised their areas for development and the transformation was in response to this. Impact of this transformation was not yet clear, but staff and partners told us this was a positive change.
Carers’ support was a key area for development, and this was reflected in data which showed significantly worse performance than national averages in several areas. The local authority had taken steps to improve their unpaid carers offer including a further commissioned carer support partner. A coproduced carers strategy was being developed but the current strategy was out of date.
Waiting lists delayed people accessing support. The local authority had reduced their waiting lists, including by outsourcing backlogs. Staffing had been increased across social care significantly to help manage workloads, which included frontline teams, but some staff told us capacity was still an issue.
Information was not always accessible. This included supporting people with reasonable adjustments, so information was available in a suitable format. Support for people with sensory impairments was limited, although the local authority was taking steps to increase this. The front-door of adult social care had moved to localities to streamline contact processes and there were plans for physical hubs to support people to access information.
There was a strength-based and outcome focused model. Staff feedback and assessments broadly reflected this approach. Access to care provision was limited and this had some impact on people’s choice over services. The local authority had strong working relationships with neighbouring local authorities to access out-of-borough services.
Coproduction to influence change was recognised as an area for improvement. Partners told us support and investment for coproduction had been limited and there was mistrust from communities following, for example, a cancelled coproduced project. The local authority was taking steps to address this, and this was reflected in strategies and processes such as specific coproduction groups.
Safeguarding processes reduced the risk of abuse and/or neglect to people. Communication with people and partners was inconsistent following referrals but staff understood the need to make safeguarding personal. Transitions pathways from Children’s to Adult services were being transformed to support earlier contact with young people and more robust processes.
The local authority’s integrated teams performed strongly. The Multi-Agency Care and Coordination Team (MACCT) offered people a coordinated service which reduced hospital admissions and supported independence. Similarly, reablement services were performing well and reduced readmission to hospital.
Senior leadership was visible, supportive of staff, and worked together to support a positive culture. There was a positive workforce development offer with opportunity for progression. Quality assurance systems supported the local authority to improve their systems and processes.